

Category Archives: Sports Medicine Tips
Orlin & Cohen Sports Medicine Tips and Tricks: Skin Lesions
![]()


Orlin & Cohen Sports Medicine Tips and Tricks: Shin Splints & Stress Fractures

Orlin & Cohen Sports Medicine Tips and Tricks: Foam Roll

Orlin & Cohen Sports Medicine Tips and Tricks


Orlin & Cohen Sports Medicine Tips and Tricks: Concussions
This week’s Orlin & Cohen Sports Medicine Tips & Tricks on Section XI is about concussions, the invisible injury.
![]()
Does Your Child Have a Sports Injury?
Does your child have a sports injury?
Northwell Orthopedics is here to help throughout every season.
Contact (833)-9-SPORTS
![]()
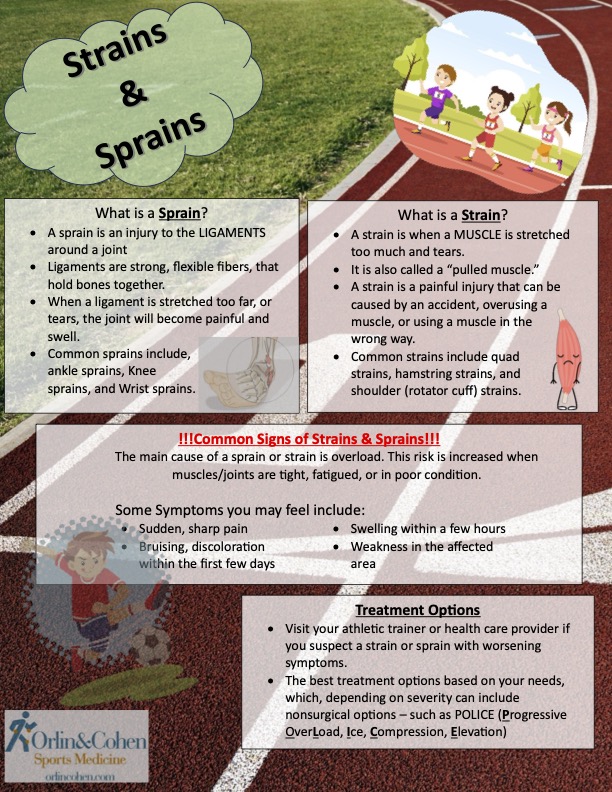
Orlin & Cohen Sports Medicine Tips: Sprains & Strains
This week’s Sports Medicine Tips & Tricks topic is Strains & Sprains.
It dives into the differences between common recovery treatments and what to do if you ever find yourself with one.
Common Knee Injuries Occurring During Spring Sports
 By James M. Paci, MD
By James M. Paci, MD
As the spring sports season moves forward, it is a great time to discuss common knee injuries one may encounter. Sports such as lacrosse and track and field require student athletes to engage their knees in both bending and rotational movements. In some situations such motions may become excessive, leading to injury. Knee injuries may cause symptoms including pain, swelling, locking, buckling or instability. Commonly injured structures include meniscus cartilage, ligaments and articular or joint surface cartilage.
The Knee Joint
The knee joint is a hinge joint allowing for the straightening and bending of the leg, however due to its shape and ligaments also allows for rotational motion as well. Noncontact injuries and contact injuries may cause the knee to bend beyond its normal motion or via direct blow cause injury to the structures making up the joint. The end of the thigh bone (femur) and the top of the shin bone (tibia) meet to make the joint and are covered with a smooth white surface called articular cartilage. Acting as cushioning gasket type structures, the medial (inside) and lateral (outside) meniscus cartilage discs are C-shaped structures which help to marry the more rounded femur to the flatter tibia. This helps to spread the normal forces that the knee sees safely across the joint. The many ligaments of the knee help to make the joint stable to all of the forces it may see. The most commonly injured ligaments are the anterior cruciate ligament (ACL), and the medial collateral ligament (MCL). Other ligaments that may be injured include the posterior cruciate ligament (PCL), the lateral collateral ligament (LCL), the posterolateral corner ligaments (PLC) and the medial patellofemoral ligament (MPFL).
Meniscus Injuries
Meniscus tears often occur in isolation through a squatting and twisting mechanism, encountered in sports such as wrestling, in combination with ligament tears, or due to instability from untreated ligament injuries. Meniscus tears generally present with pain along the inside or outside of the knee and swelling. In some situations they may cause the knee to lock, resulting in a loss of range of motion in bending or straightening the knee. A locked knee in an athlete caused by a meniscus tear generally requires urgent surgical intervention. Athletes with acute onset of knee locking should seek evaluation by an orthopedic sports medicine specialist in a timely manner. Depending on the pattern of a meniscus tear and its location nonsurgical or surgical management may be warranted. Based on the type of tear and findings at the time of surgery partial meniscectomy (trimming) or repair (sewing back together) may be performed. Return to play varies based on treatment and can take several weeks to upwards of six months for a complex repair.
Ligament Injuries
Knee ligament injuries may occur from both contact and non-contact mechanisms. A ligament sprain results from when the knee moves with a force beyond the strength of the ligament. Mild sprains may cause pain without instability, while complete tears will result in instability or joint looseness often causing knee buckling.
The medial collateral ligament (MCL) is on the inside part of the knee and supports the knee in side-to-side motion. When injured in isolation, it is usually managed without surgery. Injured athletes should be prescribed a brace and physical therapy. Anti-inflammatory medications or Tylenol may be used in addition to ice for pain and swelling. Return to play after MCL injury ranges on average from 2-12 weeks depending on severity and associated injuries.
The anterior cruciate ligament (ACL) is one of the two central ligaments of the knee, the other being the PCL. The ACL gives anterior-posterior as well as rotational stability to the knee due to its oblique orientation. When the ACL is torn, the knee often swells significantly becoming painful to walk on. Athletes suffering an ACL tear often report feeling or hearing a pop or snap at the time of injury. Unfortunately, ACL tears are often accompanied by additional injuries to ligament, meniscus or articular cartilage tissues. Complete ACL tears generally require surgery to return to sports. Depending on the location and type of tear, athletes undergoing ACL surgery will be candidates for ACL primary repair, partial or complete reconstruction using other tissues to create a new ligament. When undergoing reconstruction, based on the most up to date evidence, allograft or donor tissue grafts should be avoided in young athletes due to the significantly greater risk of retear or failure when compared with using an autograft, or one’s own tissue. Common autografts include patella tendon (kneecap tendon or bone patella tendon bone), hamstring tendon and quadriceps tendon. The benefits and risks associated with each graft type should be discussed in the context of the athlete’s sport and life goals prior to graft selection. Not every graft is best for every patient and long term results are very similar for all. Both before and after surgery, athletes undergoing ACL surgery should expect to participate in a long period of physical therapy followed by a structured return to play program. While many myths exist based on professional athletes amazing recoveries, athletes should expect to return to sport between 6 and as many as 12 months after ACL surgery. In the unfortunate case of revision ACL surgery, return times may be even longer.
Articular or Joint Surface Cartilage
The smooth white covering on the ends of the thigh (femur) and shin (tibia) bones and under the kneecap (patella) is called articular cartilage. Along with the normal joint fluid in the knee, this highly specialized surface allows our joints to move freely with very little friction. However, injury to this surface can cause pain, swelling, catching, popping and locking. While arthritic conditions can cause generalized loss of this surface over time, acute athletic injuries may cause localized cartilage defects. These defects are akin to potholes in a highway. These potholes are often accompanied by a loose body or floating piece of cartilage or bone within the joint which may cause secondary injuries. While attached cartilage injuries may be treated with rest, limited weight bearing and therapy, detached or loose isolated cartilage injuries usually require surgical intervention. Surgical interventions for these injuries include simple debridement for smaller areas, direct cartilage repair, single stage cartilage replacement using one’s own cartilage from a different area of the same knee, single stage cartilage replacement with donor cartilage, or multi-staged cartilage replacement using one’s own cartilage or donor cartilage. While a simple debridement of clean up may allow for return to sport in several weeks, large donor cartilage replacements have been shown in NBA players to take up to 12-24 months for full return to sport.
Summary
Knee injuries in athletes should be evaluated quickly by a sports medicine expert in order to minimize time missed participating in one’s sport. We are very fortunate on Long Island to have terrific athletic trainers in our schools who are an amazing resource to use for initial evaluations, on site injury management and injury prevention. Sports medicine fellowship trained primary care physicians and sports medicine fellowship trained orthopedic surgeons are experts in the diagnosis and management of sports related injuries, including injuries to the knee. The experience and skill of this select group of physicians allows them to help athletes facing injury get back on the field, mat or court in a safe and timely manner. Our fellowship trained experts at Orlin & Cohen Sports Medicine are available to help seven days a week.